
This blog is the first of two posts that will take a deeper look into Virginia’s efforts to integrate the 988 hotline with the behavioral health crisis services continuum.
**This blog contains information and statistics on suicide and mental health. If you or a loved one are experiencing a crisis or need mental health resources, contact the National Suicide Prevention Lifeline at 1-800-273-8255 (en Español: 1-888-628-9454; deaf and hard of hearing: 1-800-799-4889) or the Crisis Text Line by texting HOME to 741-741.
On July 16, a new three-digit national hotline–988–will launch to connect callers with trained counselors through the National Suicide Prevention Lifeline to provide 24/7 call or text support for anyone experiencing a mental health crisis or in need of suicide prevention services. Though the hotline is administered through the national Lifeline, calls to 988 will be routed based on area code to regional crisis call centers that can connect individuals with crisis and emergency services that are available in their local communities.
Virginia is utilizing the national 988 hotline implementation as an opportunity to link the three-digit dialing to the broader behavioral health crisis services continuum that is being developed across the state. Eventually, this will mean that more young people and their families will have access to mental health professionals responding to a crisis instead of law enforcement. This is especially important given the compounding traumatic effects of the COVID-19 pandemic, systemic racism, LGBTQIA+ discrimination, and gun violence in this country.
Suicide is the second-leading cause of death among young people aged 10 to 24. However, deaths from suicide are only part of the problem. Each year, approximately 157,000 youth between the ages of 10 and 24 receive medical care for self-inflicted injuries at emergency departments across the U.S.
The Centers for Disease Control reported that during 2020, mental health–related emergency department visits among youth aged 12 to 17 increased 31% compared to 2019. Specifically, emergency department visits for suspected suicide attempts among 12 to 17-year-old girls were 50.6% higher in February to March 2021 than during the same period in 2019; among boys aged 12 to 17, such emergency department visits increased 3.7%.
In Virginia, the percentage of students who experienced feeling sad for two weeks or more increased significantly from 2011 (25.5%) through 2019 (32.4%). And among those who reported feeling sad for two weeks or more, 39.1% reported that they considered attempting suicide, 29.5% made a suicide plan, 18.0% attempted suicide and 4.9% made an injurious suicide attempt.
The pandemic is deteriorating children’s mental health to new lows, with more than 25% of high school students nationally having reported worsened emotional and cognitive health.
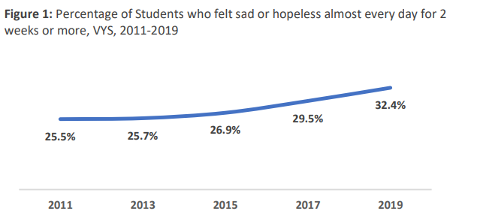
Figure 1: Percentage of Students who felt sad or hopeless almost every day for 2 weeks or more, VYS, 2011-2019
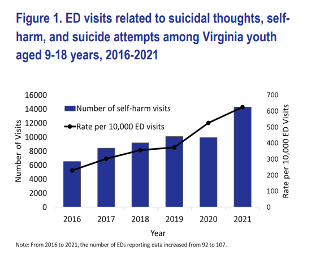
Figure 1. ED visits related to suicidal thoughts, self-harm, and suicide attempts among Virginia youth aged 9-18 years, 2016-2021
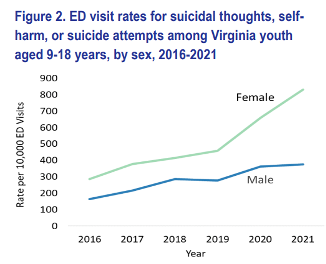
Figure 2: ED visits rates for suicidal thoughts, self-harm, or suicide attempts among Virginia youth aged 9-18 years, by sex, 2016-2021
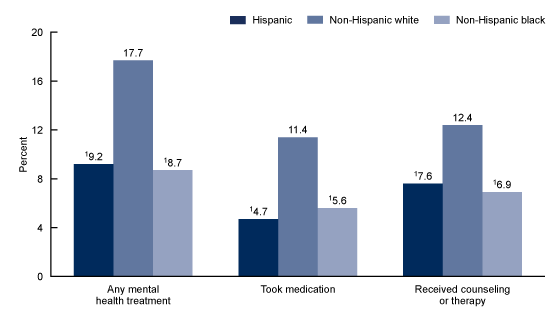
Although rates of mental health problems are not statistically different by race, the rate at which children of color receive mental health care is much different than white children. A National Center for Health Statistics data brief reported that non-Hispanic white children (17.7%) were more likely than Hispanic (9.2%) or non-Hispanic Black (8.7%) children to have received any mental health treatment in the past 12 months.
As noted in Voices’ Children’s Mental Health Discussion Paper, “systemic barriers such as eligibility criteria for health insurance and accessibility of services contribute to lower participation among Black and Latinx children. A history of racism and disinvestment in communities of color have made mental health services less accessible for children of color by geography, cultural fit, and language.”
LGBTQIA+ youth also often lack access to affirming spaces, which include health care and mental health care services. The Trevor Project’s 2022 National Survey on LGBTQ Youth Mental Health reported that 60% of LGBTQIA+ youth who wanted mental health care in the past year were not able to get it. Some of the reasons youth cited for wanting care but not having access include fear of discussing mental health concerns (48%), concerns with obtaining parent/caregiver permission (45%), fear of not being taken seriously (43%), and lack of affordability (41%).
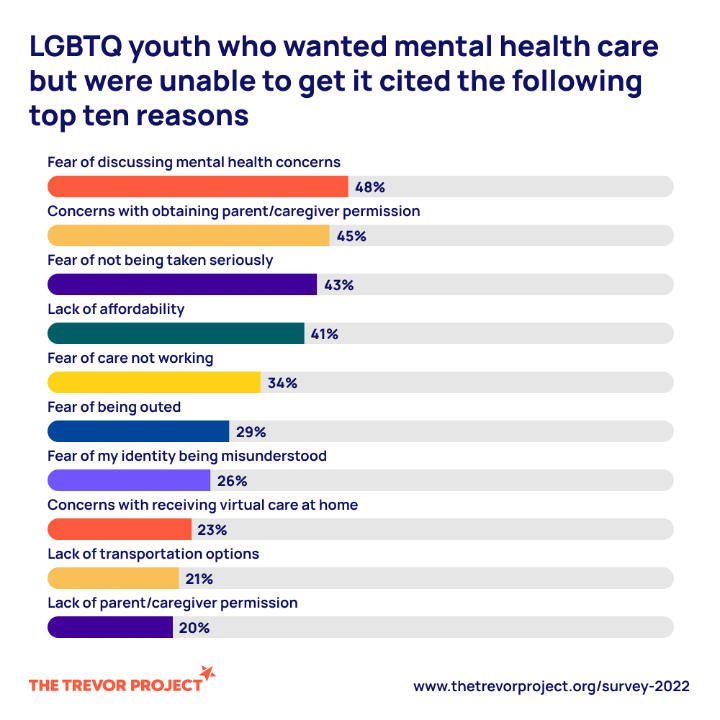
LGBTQ youth who wanted mental health care but where unable to get it cited the following top ten reasons.
Of the LGBTQIA+ youth aged 13 to 17 that were surveyed, 73% reported symptoms of anxiety and 67% reported symptoms of depressive disorder in 2020. Almost half of those youth surveyed seriously considered attempting suicide in the past year.
These statistics demonstrate the clear need for appropriate and effective mental health services for young people. Lack of access can lead to serious and lasting impacts across all areas of a child’s life. Ensuring that emergency services are accessible, unintimidating, and culturally competent will take creating programs like the 988 hotline and implementing them with full funding and public support.
As lawmakers work to streamline Virginia’s mental health and behavioral health system, Voices is focused on opening these services to all our communities and addressing past harms in the way of healing.
Stay tuned for more on the 988 hotline and children’s mental health.
Read More Blog Posts