
For years, communities have advocated for diverting mental and behavioral health calls away from law enforcement and for states to adopt a comprehensive crisis response system. Now, that dream is beginning to come to fruition. On July 16, the National Suicide Prevention Lifeline transitioned to the three-digit number 9-8-8. While this transition was initiated by legislation at the federal level, states are responsible for the rollout and linkages to their crisis response systems when the caller’s needs cannot be resolved over the phone. Virginia has been working on a rollout behind the scenes to link the lifeline to crisis response services that are currently being designed and implemented by state agencies and stakeholders.
The commonwealth’s plan for minimizing emergency room visits for mental health crises and providing an alternative to calling 9-1-1 is to link the crisis call centers with regionally focused resources by integrating mobile crisis response alongside the Marcus Alert protocols. However, at this moment, this is simply the goal and not the reality. The development and implementation of Virginia’s behavioral health crisis system has been a piecemeal approach, and is not yet fully prepared to deliver comprehensive, trauma-informed, and culturally responsive services to meet individuals’ mental health needs—specifically the needs of young people
The Surgeon General sounded the alarm in December 2021 by issuing an advisory on the youth mental health crisis. Despite widespread awareness, young people’s mental and behavioral health needs are often an afterthought or part of “phase two” when developing programs and services. Current resources dedicated to young people’s behavioral health make up less than 10% of Virginia’s overall behavioral health agency budget. The lack of sufficient funding and resources further the disparities that historically marginalized communities face in accessing support and services.
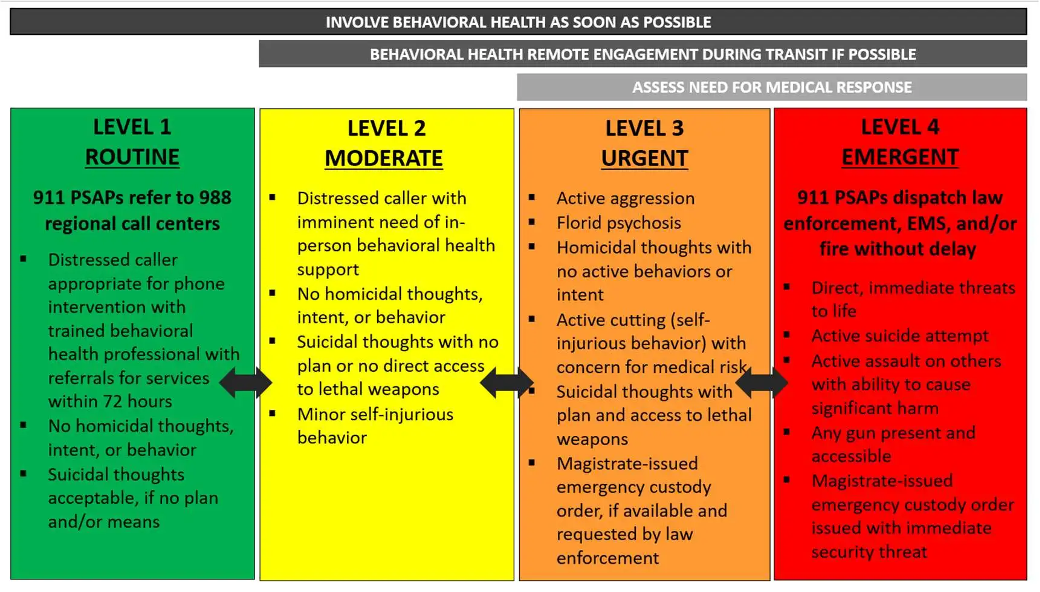
Due to the inconsistent mental health crisis services across regions, law enforcement is often the first point of “care” for mental health emergencies, especially for Black, Latinx, Indigenous, and LGBTQIA+ youth. While most calls to 9-8-8 can be resolved during the call, some crises will require an in-person response based on a four-level call matrix.
This new entry point for mental health support is supposed to be an alternative to law enforcement response, but a new law allows 89 of Virginia’s 133 localities with 40,000 or less residents to opt out of two protocols under the Marcus Alert System. This means that for those living in one of the 89 localities that are not required to implement all Marcus Alert protocols, an attempt to get in-person crisis support may still result in law enforcement, with or without Crisis Intervention Training, responding to your call. The criminalization of youth crises often results in further traumatization. This experience can intensify their crisis, compromise their treatment, and make them and their families less willing to call for help if another crisis occurs. Far too often children and families are met with a response that is not suited to meet their immediate or long-term needs.
At a time when young people need support the most—while their worlds have been turned upside down by COVID-19—we must ensure there are providers and services in place to provide access to timely, culturally responsive services, and address social determinants of health to support children and families’ overall wellbeing. This requires investments from lawmakers and interagency collaboration.
While all these recommendations are not immediate and some are considerations for future policy, Voices for Virginia’s Children suggests the following key recommendations:
Voices will continue to advocate for increased access and improved coordination of quality mental health services for all children in Virginia, regardless of where they live or at what point they seek mental health services. The future wellbeing of our state depends on how we support and invest in the next generation.
To learn more about Virginia’s plan for crisis system transformation, visit these resources: Virginia’s Crisis System Transformation and Marcus Alert and STEP-VA.
Read More Blog Posts