Investing in Health Equity During the 2024 Legislative Session
Posted: - By:Emily Moore
As we enter the 2024 legislative session, we are also nearing the end of Medicaid Unwinding, which began in March 2023. Over 81,000 children and youth in Virginia have been terminated from Medicaid coverage during unwinding—many for procedural reasons rather than ineligibility—adding to the roughly 87,000 children in Virginia who are uninsured due to administrative guidelines and barriers, language and literacy barriers, and immigration status requirements.
Lawmakers have an opportunity this session to prioritize expanding health care coverage and equitable access to health care services in all communities. Young people and their families deserve a health care system that:
Promotes the improvement of health outcomes through preventative care;
Provides culturally responsive and gender-affirming care; and
Prioritizes a workforce that is reflective of Virginians.
A deep dive into the data shows the stark inequities in health care coverage depending on a child’s immigration status. While children who are citizens have an uninsured rate of 3.7%, Virginia children with undocumented status are estimated to have an uninsured rate of 48%.
Undocumented and uninsured children currently navigate a patchwork safety net system to access health care services. These systems are difficult to navigate and are costly to families and the state. Investing in the health of children and youth now means a healthier future.
“Cover All Kids” funding would establish a health coverage program, which would mirror Medicaid/FAMIS, available to children from low-income families regardless of immigration status.
Maternal and Infant Health
As reported by the Virginia Maternal Mortality Review Team, Virginia’s maternal mortality rate more than doubled between 2018 and 2020 from 37.1 deaths to 86.6 deaths per 100,000 births, and Black women continue to experience higher rates of pregnancy-associated deaths compared to their white counterparts (80.5 vs. 53.9, respectively). Despite Virginia’s progress in supporting policies to address disparities in maternal health care—such as FAMIS Prenatal Coverage, 12 months postpartum continuous Medicaid coverage, and Medicaid benefit for doula services—systemic issues and racial disparities continue to persist, leaving many birthing people without access to the quality maternal health care they deserve.
And even with increased maternal care coverage, the availability of birth hospitals, clinics, and providers is heavily impacted by geography.
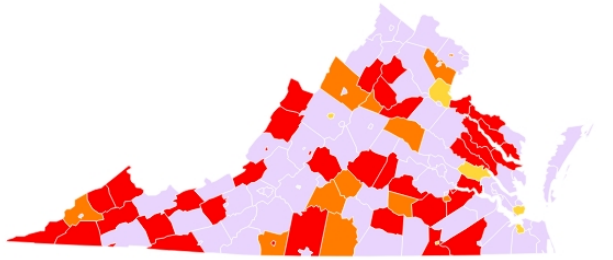
March of Dimes reported that in Virginia, 30.8% of counties are defined as maternity care deserts and 14.8% of birthing people had no birth hospital within 30 minutes from them. Rural communities suffer most from maternal care deserts, with only 1.8% of maternity care providers practicing in rural counties in Virginia.
Policies that expand maternal care and birthing options will continue to provide birthing people with autonomy and choice throughout pregnancy and during and after birth. Expanding care options, education, and capacity around pregnancy and birth are essential to reducing maternal mortality rates.
Funding to sustain the increasing cost of administering Population Health Surveys, specifically the Behavioral Risk Factor Surveillance Survey (BRFSS), Virginia Youth Survey (VYS), and Pregnancy Risk Assessment Monitoring System (PRAMS), and support for the oversampling of priority populations. Funding shall also be used to support the Population Health Survey Unit Lead position.
Item 285 #10h (Del. Hayes) | Item 285 #2s (Sen. Locke) | Dept. of Health Professions | FY25: $50,000
Requires the Board of Medicine to establish a continuing education mandate of unconscious bias and cultural competency training for all licensed medical professionals service individuals who are pregnant or may become pregnant.
Establishes the Fetal and Infant Mortality Review Team to develop and implement procedures, including collecting and reporting triennial data, to ensure that fetal and infant deaths occurring in the Commonwealth are analyzed in a systematic way.
Funding to promote engagement in maternal and child health initiatives in Virginia private acute care hospitals, including implementing Title V block grant initiatives and data analytics programs related to advancing health equity and reducing maternal health disparities.
SB 250 – directs the Department of Medical Assistance Services to modify the state plan for medical assistance to include a provision allowing for reimbursement under certain conditions for remote ultrasound procedures and remote fetal non-stress tests.
Workforce
Virginia is experiencing significant shortages of health care providers across many of our health care settings—from pediatrics, to primary care, to hospital settings. According to a study completed by the Virginia Health Workforce Development Authority, 102 of 133 Virginia counties and equivalents are federally designated primary care Health Professional Shortage Areas (HPSAs), which impacts 29% of Virginians. Workforce challenges lead to inequitable access to health care services and disparities in health outcomes.
Voices is supporting and advocating for budget amendments this session that will improve reimbursement rates for providers and will address the recruitment and retention of a diverse health care workforce.
Governor’s Proposed Budget Items:
Enhance Nurse Preceptor Incentive Program | VDH | $6 million across the biennium
Establishes Earn to Learn Nursing Education Acceleration Program | VDH | $8 million across the biennium
Additional support for Nursing Scholarships and Loan Repayment Program | VDH | $1.87 million across the biennium
Item 288 #11h: FY25: $21.5 million GF / $45 million NGF; FY26: $28.2 million GF / $45 million NGF
Item 288 #15s: FY25: $21.5 million GF / $45 million NGF; FY26: $21.5 million GF / $45 million NGF
Provides funding to increase Medicaid reimbursement rates for services provided by primary care physicians, pediatricians, and psychiatrists by five percent.
Preserves access to 100+ state-employed Community Health Workers at risk of losing their jobs beginning July 1, 2024.
Item 285 #13h (Del. Tran) | Dept. of Health Professions | FY25: $50,000 NGF; FY26: $50,000 NGF
Permits the Board of Medicine to issue a provisional license to a physician licensed in a foreign country for no more than two years, and a subsequent renewable two-year license if the physician practices in a medically underserved area. After two years of practice, a physician licensed in a foreign country is eligible to apply for a full, unrestricted license to practice medicine.